Interview with Steve Sacks, Founder/Director at Osler Technology
Most of us using Salesforce use one or more AppExchange Apps to supplement and expand the functionality available to us. Apps range from small point solutions, such as address validation to the larger apps that address a need such as document generation (e.g. Conga) to Apps that sit on top of Salesforce that are focussed on the needs of a particular industry, such as Veeva for Life Sciences.
Have you ever wondered what exactly is involved in getting an App listed on the AppExchange? The process from having an idea to development to release?. For Dr Todd Fraser, an idea was born when on one of his regular retrieval missions, he reflected on why his retrieval pilot was required to perform supervised procedures every 3 months and re-certification every 12 months, but the same was not expected of him as a medical specialist. Osler Technology was started, with a focus on building a clinical performance App.
The vision of the Osler app is to:
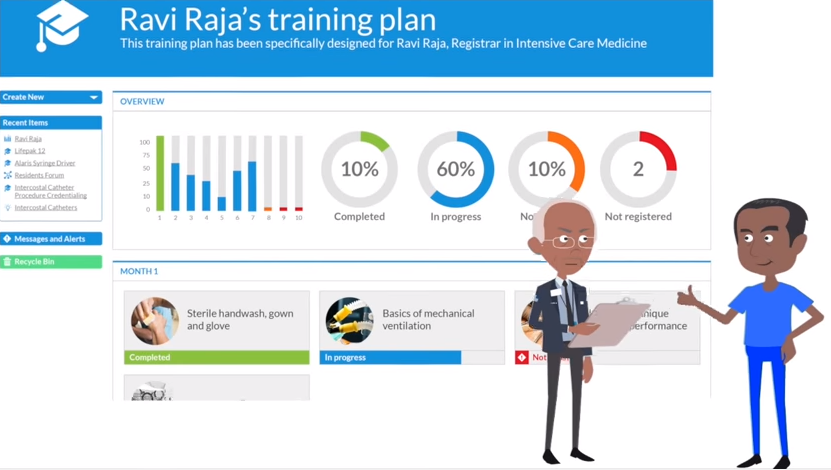
- Allow acute care clinicians to manage and track their certifications for performing procedures
- Provide a clinical & procedural report card for students, doctors, nurses and paramedics to record, measure and improve performance
- Deliver interactive, patient focused learning
- Create a Knowledge Base, a concise and trusted multimedia encyclopedia of acute care medicine
- Establish an Osler Community to enable sharing of insights & knowledge, through open collaboration between members of the worlds largest Acute Healthcare community.
Steve Sacks is one of the founders and directors of Osler technology, that brought an idea to life on the AppExchange. I spoke to Steve Sacks to find out what his experience was, going from Idea to AppExchange.
Q: Can you explain why there is a need for this App and the opportunity you saw?
Steve: There is really no re-validation process that occurs for medical specialists. The concept is starting to get some momentum and there’s some basic re-validation now required in UK. The Australian government is going through a process with a series of white papers and working groups about what to do with the re-validation in Australia, but for the most part, there’s very little objective proof of competence of re-validation that is required.
The statistic are amazing, In the US something like 500,000 people a year are dying because of adverse events that are avoidable in hospital. But because it happens one at a time, it’s not like a plane crash when 200 people die at once – it’s kind of an insidious problem that nobody’s really tried to solve it on a wholesale scale. Of course the medical industry is quite protective and insular in that respect, generally being pretty afraid of that kind of transparency.
Q: So who is the solution aimed at?
Steve: So, there’s two angles to it. The focus starts with learning in a hospital part, where the unit manager of an intensive care unit or an emergency unit, ideally wants to know who of his or her staff are competent to perform what and figure out training paths that will help them get the skills that they need and at the same time be able to monitor complication rates and some of the other procedural activity that might indicate where they’re having problems and can intervene to improve it. Typical clinical systems capture that information somewhere, but it’s very patient-centric, not really clinician-centric, and it’s surprising how little visibility that a unit manager has to procedural activity and where there are problems and they have virtually no visibility into what a clinician has either self assessed or gone through a process to acquire a competency in that procedure.
The AppExchange product is more of a hospital focused solution. We’re exploring how to go about an individual model, one of the challenges of course is that Salesforce has not historically been a business to individual solution. Their whole mindset is geared towards selling to enterprise.
Q: Why was the Salesforce Platform selected?
Steve: The ability to quickly stand up a prototype of the app, a secure & robust infrastructure, and built in collaboration capability were all contributors. Also, one of the other founders was involved in many of the early enterprise deployments of Salesforce CRM, so was familiar with both the capabilities of the platform and the potential benefits of having Salesforce as a corporate partner. We were also aware the Salesforce was in the process of increasing their focus in Healthcare (which has culminated in the launch of Health Cloud recently)
Q: How long did the App take to develop?
Steve: The first prototype was developed in 6 weeks. After meeting and demonstrating to unit managers and senior clinicians at about 25 hospitals, an additional 8-10 weeks of development was done to arrive at an MVP (minimum viable product) to start the first hospital trial. Since then development of both functionality and learning content has been ongoing to arrive at a commercial release.
Q: What challenges did you face along the way?
Steve: Commercially, the process to become an ISV with Salesforce is quite long. It took about 10 months from the time we first approached Salesforce with the idea to having our partnership approved.
Technically, we started with trying to use Salesforce1 as the framework for our mobile capability but ultimately determined that performance was not adequate for our user based and the control we had over the app was too restrictive. We’ve redeveloped the mobile environment as a hybrid app with a web app inside a native container for iOS and Android.
‘Cloud’ is still a pretty new concept to healthcare providers. WiFi is patchy in many hospitals and many desktops are still running Windows XP and old versions of Internet Explorer.
Q: I am interested in the learning and the knowledge part of the App, I wouldn’t have thought of that in the first instance as being a natural fit with the functionality that Salesforce delivers. That’s something that you needed to build in and add on, and how did you manage that?
Steve: For the learning aspect, what we ended up doing is taking a Salesforce app called Almond, which is effectively a learning management system. I wouldn’t call it fully fledged one, but it’s probably got 80% of the functionality that Cornerstone, Moodle or other commercial LMS have. So, we’ve taken that base code and had done a bunch of modification and changes to it to support what we needed and we’ve built a whole set of immersive e-learning content, focused on the junior doctor curriculum, and we’ve done that in Articulate, which is a tool for building e-learning modules and we’ve built that into the platform.
We linked it to the whole procedure certification process which is the combination of online learning, and then performance of actual procedures or simulated procedures performed under supervision where the supervisor signs you off as being competent. There are quizzes built in and you perform a number of required procedures under supervision then you get an Osler certification which is a measure of your competence in performing that particular procedure whether it’s inserting in central line, or a chest drain, or whatever it happens to be.
The knowledge pieces we haven’t done yet, we were looking at Salesforce knowledge for that, but I don’t know if that’s the right solution and we won’t probably start on that until a little bit later.

Q: The first prototype is delivered in six weeks, can you explain how that worked, did you have a team, were you working with some developers?
Steve: Yes, for the first round, we were just working, we have one developer, he was doing much of a build and I was doing the design with him and testing it and so forth. Based on sort of thoughts and initial ideas, you know the first round was pretty straight forward to knock together, and that gave us something to go around to the hospitals and demonstrate the concept.
Q: And I see some hospitals were listening?
Steve: We saw 25-30 hospitals in that first round, got some interest, enough to make it worth investing a bit into building that out so we could have it deployed it in a user environment, and for that we used some off shore resources as well and that took another couple of months.
That got us to the point, of an MVP that we started trials with 2 hospitals in August or September… and started iterating on the solution based on their feedback The trials are still going. We approached Salesforce in March or April, about the ISV program and our local AE (Account Executive) submitted the internal business case in June or July and then it wound its way through the approval process until, I guess it was December, or late November when we finally got approval to join the program. By that time, we had a few iterations of the product functionality that we submitted into security review in December, and then in January, we signed the contracts and by late January we cleared the security review, and then we listed it in the AppExchange about three weeks ago.
Q: So were you surprised by the time it took?
Steve: Not after hearing what everybody else told me about how long it takes… You know, it’s a long and somewhat blackbox process which I know the Salesforce is trying to streamline with some of the new leadership in the program that have joined in the past few months. I think that’s one of their strong focuses, but everyone we’ve spoken to took close to a year from a concept to getting an approved ISV contract.
Q: Is there any distinction between a small app and a more substantial app in terms of the process that you need to go through?
Steve: Not that I’m aware of – there are two programs… There’s the embedded platform OEM program which we’re part of where you’re essentially just using the platform to build out applications and there’s the other one, where you’re essentially just building an extension on the CRM… So with the OEM embedded we’re essentially reselling the force.com platform with our app. With extending CRM, you’re essentially selling an app that’s sitting on top of somebody’s existing CRM license so you’re not selling the platform… So there are two different streams but I think the process is pretty much the same in complexity and duration.
Q: That’s surprising because if you think about a very specific point solution such as something that sits on top of the Sales Cloud, something simple like round Robin case assignment that’s just a simple sort of add-on I would have expected that would be a much more streamlined process to get that sort of thing approved?
Steve: If it’s a free app I think it’s slightly simpler, but, even I look at something like a schedule app which is an add-on to a CRM, it would have a similar duration.
Q: You mentioned a challenge for using Salesforce1 where you found the performance was not adequate?
Steve: Yes, so in the hospital environments and probably in most other, if you want to log some sort of activity that you’ve done, some sort of procedure or whatever.. You you have to be mobile because those people don’t have offices for the most part, and so we started down the path of building out the functionality in the Salesforce1 framework, out kind of workflow required us to build custom pages. We couldn’t use the standard page layouts and we found that Salesforce1 the response time was just too slow. So we went down that process, abandoned it and I guess in about November we started rebuilding that as a single page web app living in a container on both iOs and Android and the performance is much better for us.
Q: So you have an iOS app and inside of that app you have a page that connects to Salesforce?
Steve: Correct.
Q: And because you’re not using the whole Salesforce1 framework and you’re basically doing the API calls for example…
Steve: Well it’s an HTML5 app… It’s using the angular.js framework so it’s still in effect a Visualforce page marked up with HTML but it allowed us to load the whole app in one pass and the responsiveness is much better.

Q: The last question I have was just what were the lessons learned with the AppExchange review process and assessment… You said you already had the expectation that it wasn’t a quick process… But were you prepared in terms of any feedback or any questions or concerns that came back during the process. If you were to do it again would you do it any differently?
Steve: Because the process is a bit of a black box at the moment… I probably would have asked more questions about the exact steps involved. Currently there isn’t a standard way that you present your case… while there are some templates to submit for basic information, it’s still a maturing process. So I’d probably would have asked a lot of questions about exactly what they would need along the way.
Q: And the relationship with the AE, how important is that… I guess the better the relationship, you probably would have had more information depends if the AE had gone through the process as well…
Steve: Yes, your AE is your primary point of contact and is your champion who’s going to battle for you inside Salesforce to get it up. So you need to convince that person that it’s worth the effort and investment in their time, which I think we’ve done a fairly good job of. In our case, as a standalone app in a new space, you can’t expect to get a lot of support elsewhere in the organisation so it’s important to make sure that relationship is strong.
When it comes to the Security Review, in retrospect, what we probably would have done better is thought more, earlier, on how to structure our code using the security guidelines that salesforce provide… We’ve certainly found a few missing bits when we got close to the time that required revisiting aspects of the code and implementing extra security checks that we hadn’t done in the first pass.
When it comes to security review… I mean… In retrospect, what we probably would have done better is thought more earlier on about structuring our code using the security guidelines that salesforce provide… We’ve certainly found a few missing bits when we got close to the time that required… not recording but building an extra security checks that we haven’t done in the first pass… Much of it required a bit of an overhead.
Q: So it requires substantial time and investment to get the OEM type application over the line and that might be may be difficult for situations where people aren’t very well structured and organized and have all that time available… I guess I’m thinking about the opportunities where individual developers or people that have an idea for an App It is quite a substantial undertaking right?
Steve: It does definitely require a substantial amount of investment in time to get it across the line… no question. And it might be a little bit easier for the VAR apps but yes, you need to be prepared for that and also the fact that you have to take a commercial risk. When you start, there’s no guarantee that you’ll be accepted in the program. So you could spend a lot of time building something and then find out that somewhere in the organisation it gets knocked back . So there is a commercial risk and you have to say we’re are going to continue building this product out under the assumption we’re are going to get approved and that’s where your relationship with the AE comes in because you have to make a judgement call on the feedback they’re getting and passing on to you about the level of that risk.
Talk to the AE as early as possible just to make sure that you get all the information that you’re aware of everything you can explain the idea, and to make sure that you don’t go too far down the path before finding out that you may wasted some effort… As far as that’s possible.
Q: Ok, I think that covers everything. Thank you again for your time. Sounds like there’s a really amazing opportunity in front of you…
Steve: I hope so.. we’re closing in on the first two hospitals that we started trialling last year to become our first commercial customer, and a couple of other trials started in January, so we are optimistic that we will get some traction this year. Thanks for the interview and check us at at www.oslertechnology.com !
Sir William Osler, (July 12, 1849 – December 29, 1919) was a Canadian physician and one of the four founding professors of Johns Hopkins Hospital. Osler created the first residency program for specialty training of physicians, and he was the first to bring medical students out of the lecture hall for bedside clinical training. He has frequently been described as the “Father of Modern Medicine”
What Certification are you studying for now?
Focus on Force currently provides practice exams and study guides for sixteen certifications